
 We’re back!
We’re back!
CTIS was abuzz about Digital Biomarkers and their applications in clinical trials. Several definitions floated around, but we liked the simplest one — “user-generated physiological indications captured by a device.” Many of the speakers discussed wearables, but Digital Biomarkers go well beyond that. For example, there is a pill with a heat sensor that can detect whether it has been ingested or not and reports its location in the digestive tract. A perfect example of how technology can help reduce non-compliance by remote patients in a typical clinical trial. Overall, speakers observed that technology is enabling us to capture health data reliably and in real-time. They went further to say that by identifying appropriate Digital Biomarkers as reported by these devices we will be able to overcome some of the longstanding challenges to clinical trials.
In our quest for finding efficiencies in drug development and clinical trials, one speaker presented Eroom’s Law. It is not a coincidence that it is “Moore’s Law” backwards. In lay terms, Moore’s Law states that computing power doubles every two years, as has been evident in the computing power of our wearables and mobile phones. Some of those applications were inconceivable for a consumer grade or disposable application 20 years ago!
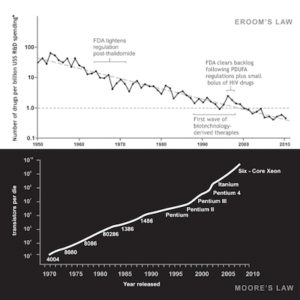
Conversely, Eroom’s Law is evidenced by drug discovery becoming slower and more expensive over time, despite improvements in technology. The skyrocketing cost and complexity of clinical trials is nothing new to those of us who grew up in this industry, but the responsibility to leverage all means available to make them come to conclusion faster and at less cost is something that must be addressed.
One speaker shared metrics that contribute to stalled studies. For example, geography remains a hindrance to patient recruitment – an even bigger challenge than exclusion criteria. Site selection to make sure that patients are close to their visits for routine procedures is a must if viewed in the traditional manner, but by utilizing wearables and telemedicine we can address that challenge and thus remove a major cost metric from studies.
 Intuitively bringing the trial to the patient rather than bringing the patient to the trial makes for better and easier interaction with the patient and therefore improved retention and compliance. Furthermore, having “live” telemetry of the patient’s physiological indications prevents chances of “missing” an episodic event that does not repeat in the study or, in worst case, does so after drug launch.
Intuitively bringing the trial to the patient rather than bringing the patient to the trial makes for better and easier interaction with the patient and therefore improved retention and compliance. Furthermore, having “live” telemetry of the patient’s physiological indications prevents chances of “missing” an episodic event that does not repeat in the study or, in worst case, does so after drug launch.
Quoting a patient advocate Linnea Olson, Lung Cancer Patient Advocate from a panel of Patient-Centric-Trial gurus from four major Pharma: “In our haste to use tech in trials we often lose the humanity in trials. Consider factors like what matters to the patient rather than fixating on what is the matter with the patient and use tech to make things easier for the patient rather than build the tech and then ask the patients to adapt to it.” This is certainly something to think about as we move ahead.
A Note from Adaptive:
In the perceived “arms race” to deploy more and more wearables and medical devices in clinical trials we have created significant fragmentation of data. Data that used to consolidate nicely in an EDC is now spread across 32+ different tools and utilities from many device vendors, Electronic medical records vendors, analytics vendors as well as eClinical vendors. Great strides have been made in combining some of the data to feed into the analytic tools that have emerged in recent years but all those results are dead-ending in the analytic tools.
 If we are to realize the true benefits of wearables, med devices and analytics we need to first create an environment that offers 360° interoperability of all the available data that not only allows us to pull the raw data, but that also allows us to take back the insights and conclusions as determined by the analytics or AI back into the data flow. This information flow modernization is a must and a required data infrastructure investment for any CRO with aspirations of surviving this arms race.
If we are to realize the true benefits of wearables, med devices and analytics we need to first create an environment that offers 360° interoperability of all the available data that not only allows us to pull the raw data, but that also allows us to take back the insights and conclusions as determined by the analytics or AI back into the data flow. This information flow modernization is a must and a required data infrastructure investment for any CRO with aspirations of surviving this arms race.